
Light and Circadian Biology #7 - Vitamin D, The Light of Your Life
Today we will cover:
What is Vitamin D, what does it do and why is it so important?
Vitamin D is an effective prevention and treatment for COVID-19
Why intracellular water and magnesium levels are so important for Vitamin D synthesis
Why you cannot generate Vitamin D even if you’re in the sun
How long does Vitamin D last in your body and what happens if you don’t have enough?
What other sources beyond the sun can enable you to generate Vitamin D?
Why is cholesterol so important and what does it do?
Why is sulphation and photoisomerization such an important process and how does it work?
Interesting facts about Vitamin D
And much more
Let’s begin!
Vitamin D 25(OH) (Calcidiol) is the inactive component of Vitamin D which is then converted in the kidneys to the active form 1,25-dihydroxy Vitamin D (Calcitriol).
The full conversion from Cholesterol all the way into 1,25dihydroxy Vitamin D is done in the biologic surfaces (Eyes, Skin, Gut and Aerodigestive tract including lungs), Liver and then Kidneys.
The conversion of VD25(OH) to VD1,25 requires a photoisomerization step which requires water in the form of intracellular hydration. Therefore, if dehydrated, this conversion will be poor and VD1,25 will be low.
Sulphated Vitamin D is created best by AM sunlight when the colour temperature of sunlight is below 6500K, in the AM. Despite UVB and IR still being present over 6500K, Vitamin D is sulphated best in the morning. In fact, any type of sulphation operates better in the morning. This is because in the morning there is a higher percentage of Red and not so much Blue light in Sunlight at that time.
How is Vitamin D created?
The process is quite a complicated quantum biologic light show, but to make it simple here’s the two major steps.
Step 1: The eye, skin, gut and aerodigestive tract (including lungs) – Photoisomerase, an enzyme in the eye that upon stimulus from UVB sunlight, takes sulphated LDL cholesterol and turns it into sulphated 25-Dihydroxyvitamin D. This links the eye, skin, and liver. 25-Dihydroxyvitamin D is the inactive form, the bank account.
Step 2: This inactive form, sulphated 25-Dihydroxyvitamin D is converted in the kidneys to be converted into the active form, 1_25-Dihydroxyvitamin D.
If the liver and kidneys are not in optimal health this generation and conversion of Vitamin D is diminished.
If the skin, eyes, gut and aerodigestive tract (including lungs) are not in optimal health the generation of vitamin D will be reduced.
The ovaries and testes as well as the brain can also covert between the two forms of vitamin D, but not to the same extent as the Kidneys and Liver.
Vitamin D’s major effect: The major effect of Vitamin D is that it modulates the immune system, given its receptor is found on T helper cells (regulator cells), the same cells that are destroyed by COVID spike protein or how HIV infection wipes them out in AIDS victims.
Low Vitamin D levels, for any reason, turn off the epigenetic switches on RNA/DNA/mtDNA genes that switch on the proper functioning of immune system protector cells which keep us free of diseases from viruses, bacteria, mould, and fungal infections.
How does Vitamin D work to support the immune system?
Innate Cellular Immunity – NKT Cells – Natural killer T cells are activated any time we are exposed to a pathogen, virus, or toxic threat. They aim to kill any cells which don’t belong and are not specific to a particular virus, but rather kill any which pose a threat.
Adaptive Cellular Immunity – TNF pathways = CD4 and CD8 T cells. These more targeted T cells are produced any time a specific virus attacks the body such as SARS-COV. In this case it will be contracted to kill any SARs-COV or related Corona viruses. T cell immunity can last for years and up to 17 years later in this study: https://www.nature.com/articles/s41586-020-2550-z
Humeral immune response – The production of antibodies (Immunoglobulins IgM, IgG) by B cells as a reaction to a cellular immune response. These antibodies are virus specific and do not offer cross-reactive defence for any other viruses other than their specific target. Antibodies can only last a few months.
The immune system is much more robust when focusing on T cells rather than antibodies. Vitamin D is a major precursor for activation of T-cells (for any disease) while poor Vitamin D levels cause the body to lose control over the cytokines storm in COVID that causes blood clot & vascular damage of the organs like kidneys, heart, brain, and ultimately death.
Vitamin D2 and D3 supplements do not operate like the D3 made from sulphated cholesterol when exposure to UV light and changed to the active neurohormone in the kidney and liver. When sunlight is used to operate the Photoisomerase step in the skin to change the sulphated cholesterol to sulphated 25 D(OH), the compound must be changed to 1, 2, 3 D3 in the peripheral tissues that have proper peripheral clock gene function under the direction of melanopsin/retinol and melatonin. In humans the major conversion occurs in the liver and kidney. Vitamin D3 made in this way in humans is not really a vitamin; it is an immunosuppressive steroid that prevents a reaction of the immune system against the MHC complex to protect you from autoimmunity. D3 and the Vitamin D Receptor (VDR) also slow the electron tunnelling speeds in the mitochondria to improve apoptosis. There is a Vitamin D Receptor (VDR) between Cytochrome 3 and 4 and 4 and 5 along the inner mitochondrial membrane. This is how it operates to block oncogenesis in humans. Human cancers all require immortality and thus apoptosis is cancer’s kryptonite.
The Vitamin D savings bank
Humans have a Vitamin D savings bank in our body. It is supported by a good protein diet and leads to a better Vitamin D level. A seasonal seafood and organ meat-based diet is an optimal choice for this bank account. It works by the liver making a protein called Vitamin D binding protein (DBP). It acts like albumin does in the blood. The vitamin D-binding protein (DBP) is a highly specific carrier for vitamin D and all of its metabolites found in the plasma. This allows us to store vast amounts of Vitamin D.
Evolutionarily, Vitamin D synthesis from cholesterol by the sunlight is thus maintained within physiological limits estimated to be 0.01 to 2.5 mg of cholecalciferol per day. 2.5 mg per day translates to 100,000 IU per day! If we are protein deficient, we do not have this ability and our stores are low in low light levels. It not only protects our Vitamin D stores, but it also prevents the toxic effects of a high vitamin D level in the blood.
1-25 dihydroxy vitamin D or Cholecalciferol is the active form of Vitamin D in the body. Humans start to store Vitamin D3 when Vitamin 25(OH)D (hydroxyvitamin D) level is above 40 ng/ml. The interesting finding is that it is only around a level of 60 ng/ml that the stores are sufficient to see us through a winter with a resultant optimal D level. This is why dietary composition is critical for immunity the further one gets from the equator. Seafood is one of the few foods high in Vitamin D levels. At the equator there are no foods with Vitamin D because the tropical sun provides all we need.
Vitamin D from places other than sunlight
Food, supplements, and phototherapy are three other places which vitamin D can be obtained. However, sunlight is by far the best and safest source.
Vitamin D from food
To get vitamin D from food, fish is a good option. Six ounces of cooked salmon has more than 600 international units (IU); this is the daily recommended Vitamin D dietary intake. Fish: Mackerel, Sardines, Salmon. Beef Liver. Pastured Eggs (yolks).
Pro Tip: Fish eyes and skin have the highest concentrations of Vitamin D.
Assuming you are living with the environment and eating organic/wild/biodynamic/raw/grass-fed and locally, nature supplements the lack of UVB light through dietary sources and storage of Vitamin D in adipose fat.
Cold stimulus is also used to sensitise all photoreceptors in your body to sunlight to capture as much available UV light as possible in the colder months if any.
Dietary sources include Fish, Eggs and Milk. The best sources are Wild Salmon and Sardines, Wild Raw Milk, Biodynamic or Organic Eggs.
In Winter, the body increases the number of immune defence cells in the blood plasma compared with any other season which increases the requirement for immune system Vitamin D.
During Autumn/Fall (Pre-winter) the body is designed to be at its heaviest. Then during winter, the body catabolises some of its fat stores which contains Vitamin D and uses this to maintain reasonable levels of Vitamin D in the blood throughout winter, assuming you have generated sufficient Vitamin D during the Summer and early Autumn/Fall. Ancient cultures likely migrated small distances during the wintertime to improve their immunity and dopamine with stronger sunlight, however as long as they lived in nature and by her rules, their bodies would have been following the path outlined above and were able to withstand a Winter whilst maintaining a reasonable level of Vitamin D.

But what if you begin winter with low Vitamin D?
Furthermore, if you are already unwell during Winter, then you would agree that recovering from this, from a Vitamin D perspective, is not easy. If you have failed to create enough Vitamin D stores in your body during the sunny months and it is now Winter with no UVB for the next 3 months, you have 3 options.
Use the cold in your environment to improve your innate immunity, eat foods containing Vitamin D and avoid spending time with unwell people.
Travel for 2-4 weeks to an environment which has UVB sunlight available to build up your Vitamin D from the natural sunlight and cholesterol in your skin whilst ensuring your mitochondria are healthy, keeping you hydrated.
Supplement Vitamin D orally or via a UV lamp/bed. This is the worst option of them all for several reasons we will get into next. IT’S NOW YOU do not support either of these options without first consulting a dermatologist or your doctor because there are contraindications and side-effects. Nature has built wisdom into your biology (as shown above) to allow for a robust immune system during winter. Instead of supplementing Vitamin D, eat seafood. Vitamin D is not meant to be supplemented independently of Vitamin A, Magnesium, Vitamin K2, and Sodium. The correct combinations of these minerals and their downstream actions are available in seafood during the winter and local seasonal food + sunlight in the summer.
What should you be aware of if supplementing Vitamin D?
When you take a supplement of Vitamin D it is akin to hiring a trainer in a gym and asking him to do push-ups for you and thinking you are getting the benefit. There is a short-term benefit for supplementation in a medical context but there is no evidence that long term supplementation works at all and this puts the dermatology idea of burying the sun and just taking pills to bed.
Furthermore, simply by supplementing Vitamin D, this throws out, Vitamin K, Calcium regulation and Vitamin A. Nature couples all these together along with melanin pigment in skin and the gut microbiome to ensure proper immune function.
When Vitamin D is created naturally from sunlight, it and sulphated cholesterol remain sulphated for much longer than with supplementation. The reason this happens is tied to the higher melatonin levels which are generally found in those who have higher vitamin D. Melatonin is what keeps them sulphated, assuming calcium is normal in the blood serum.
Vitamin D supplementation is best done in food via eating fish eyes and skin or sun-soaked mushrooms.
Logic says that before Planes - Trains - Automobiles. People did just fine at high latitudes. Why? Mostly because they lived a more outdoor existence connected to the sun and earth and ate seasonally and locally. Logically they gained 5-10lbs before Winter. Since Storage D is in fat... it's logical to release D via a ketogenic diet given carbs aren't available through Winter. Eating high fat/D foods gives you some D but not enough for serum levels to last you through Winter. You must accumulate Vitamin D during summer.
It's a very individual decision, but you can see now that it's often a wise move to spend some time away from home in the tropics if you have not been able to prepare for winter. It is prudent to aim for a Vitamin D of 60ng/ml (150nmol/L) or above prior to winter to lower ‘all-cause mortality’.
How much Vitamin D is enough?
Meta-Analysis says “A pooled dose–response curve showed that the hazard ratios declined steeply between 0 ng/mL and 30 to 39 ng/mL, then appeared to plateau at serum 25(OH)D concentrations above 50 ng/mL (Figure 3). The curve was steep at lower concentrations through 30 to 39 ng/mL, with a slight trend toward lower risk at 40 to 49 ng/mL compared with 30 to 39 ng/mL”
So, add 10ng/ml and you’re in the clear with a little vitamin D buffer for the winter.
Cité: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4103214/
My experience, I had cancer when I had a vitamin D of 37ng/ml (90nmol/L)
Everyone has VDR receptor differences which means they can tolerate different levels of vitamin D. The highest I have seen is VD OH-25 of 40 and my client had cancer. So as long as you are above that in my experience your risk of all-cause mortality is extremely low.
What if I can’t get my Vitamin D up using sunlight?
Are you spending time under the power of UVB rays and your Vitamin D is not going up? When I was living in Melbourne, Australia (37-degree south latitude), I tracked my Vitamin D monthly for 5 months from late spring to early Autumn/Fall. At the beginning I was sitting at 92nmol/L. I spent an average of 3 hours every second day in direct sunlight with 90% of my skin exposed when the UV Index was above 3. As the months wore-on my levels were very flat, never exceeding 100nmol/L. By the end of the 5 months my Vitamin D was at 95nmol/L. Why could I not get this higher? The reason for this in tissues is because the absorption coefficient or optical density in their tissues has changed. That means, that some other light frequency around them is affecting their conjugated systems from absorbing UV light. This is usually non-native electromagnetic fields (nnEMF), such as cosmic rays, gamma rays, x-rays or microwaves. That means, Wi-Fi, 4G, 5G, Bluetooth, smart meters, local distribution lines, electric fields, magnetic fields, radio frequencies, a thin ozone layer or any electrical technology device is reducing your body’s ability to synthesise vitamin D. It does this in many ways, including dehydrating your tissues, destroying the cholesterol in your skin, and interrupting normal biologic signalling by raising inflammation.
So, what did I do? I spent 3 weeks at a friend’s house 1 hour away from my house, still at the same latitude, but he had no Wi-Fi, smart meter, or cell phone tower near his house. I then followed the same protocol, 3 hours every second day in the Autumn/Fall UVB sunlight. Result? My Vitamin D levels came back at 109 nmol/L.
Chronic blue light and nnEMF exposure UNSULFATES the blood and proteins in the body. This lowers the amount of light energy that can be buried in water and the cells in your body. This makes the mitochondria energy inefficient and if it goes on long enough it will lead to leptin resistance. What do you think this implies for your ability to generate Vitamin D?
Un-sulphated Vitamin D has the ability to regulate calcium homeostasis in the blood. A low vitamin D level will result in less calcium absorption in the gut!
Unsulfated Vitamin D will also raise the amount of unsulphated LDL cholesterol in your blood while causing retinol binding protein to rise and your B2 (riboflavin) levels to fall off a cliff. If this goes on long enough melatonin, serotonin, and NAD+/NADH level at cytochrome 1 also become markedly abnormal and this indirectly slows the methionine cycle. When the methionine cycle slows down, the body becomes a net collector of heavy metals. At this point, it no longer matters if the environment is filled with heavy metals, because the body has lost the ability to detoxify them given the loss of control of the sulphation. Sulphation controls The Methionine Cycle. If sunlight is not sulphating the microbiome, then the microbiome loses diversity and becomes toxic. Riboflavin in the gut absorbs Blue Light and thus is associated with optimal gut function as the bacteria release blue light in the gut under normal function. Riboflavin does this because it has three benzene like ring structures with nitrogen associated with them. This is similar to chlorophyll and haemoglobin as they also require activation of the pi electrons (HOMO and LOMO actions) which act to make them all the perfect blue light photon trap. Did you know that all B vitamins are blue light chromophores!
Reference: https://www.youtube.com/watch?v=g_rlcavhGLs
Summary: If you have wireless radiation in your environment, it is affecting your ability to synthesise Vitamin D. If you have high inflammation levels, poor liver function or a disease like diabetes your ability to synthesise Vitamin D is diminished. If you are dehydrated, the same issue pops up. If your environment is capping your immune system health, does it seem right to waste money supplementing, mitigating the risks you are now aware of or change environments? The choice is yours.
But what if it’s winter and there’s no UVB available?
The sun in the mountains allows the body to produce Vitamin D in winter. If one is over 5,000ft above sea level, Vitamin D can be produced by the body all year round.
Above 5,000 feet altitude, there is a massive surge in UV light. Mountain living is akin to blood irradiation with UV light. UV light is capable of inducing magnetic fields and introducing magnetic flux. RBC’s absorb this because blood is a magnetohydrodynamic fluid. When UV light is absorbed by components of the blood, the light energy and information quanta can be transformed into other forms of light after collisions with things made of matter in our cells or the light energy can be changed to acoustic phonons which can carry magnetic data on for infinity because solitons have this ability by physical laws. Acoustic phonons are a form of solitons that can be programmed by magnetic energy carried in sunlight.
Vitamin D can drop fast after Summer
When sun exposure drops off dramatically, Vitamin D levels will drop very quickly too. The drop is even bigger if high heteroplasmy exists in the body. Furthermore, if the BUN/Creatinine Ratio is high, Vitamin D will drop even more sharply.
The mitochondria’s ability to make water can be interpreted through the BUN/Creatinine Ratio. When this ratio is high, Vitamin D cannot be made effectively. Because, the conversion of LDL Cholesterol to Vitamin D requires a photoisomerization step requiring water. If this water is deuterium loaded, Vitamin D will not go up. This is why Vitamin D is a great proxy for sunlight, water and nnEMF in the environment. Australia has the highest levels of deuterium in drinking water compared with almost any other country on the planet. So, my Aussie members are you ready for this… Animal fats are deuterium depleted which can substitute for poor water.
Once the water we make is optimized, it’s important to focus on high quality drinking water, which is:
Free from chemicals like fluoride and chlorine, bromine and heavy metals.
Of fresh, spring or glacial origin,
Structured by nature,
Low in deuterium and,
Blended with natural minerals, such as organic sea salt or electrolytes.
Water is fundamental to every chemical reaction in the body. Staying hydrated will allow your body to perform.
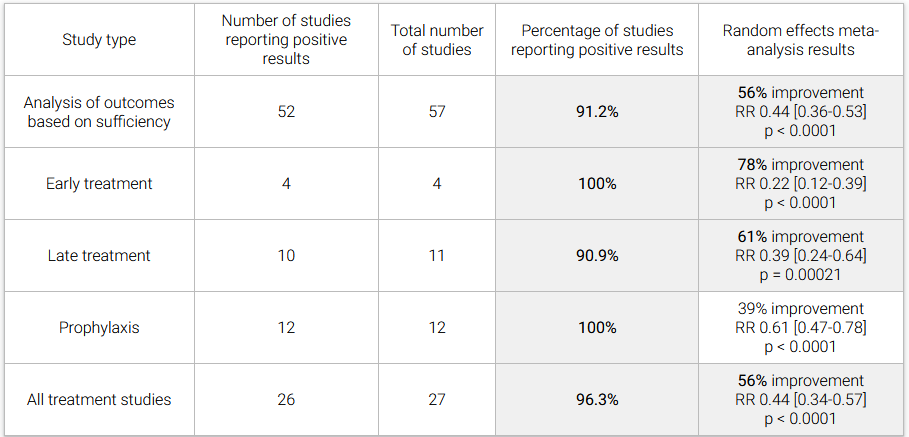
Vitamin D in treating COVID-19
Source: https://vdmeta.com/
Conclusion: 96% of 27 vitamin D treatment studies report positive effects (15 statistically significant in isolation). Vitamin D is an effective treatment for COVID-19. Random effects meta-analysis of the 27 treatment studies to date results in an estimated reduction of 56% in the effect measured, RR 0.44 [0.34-0.57].
As at June 2021 – Studies using Vitamin D on COVID-19 patients:
So why have our “experts” been telling us to stay inside, isolate, quarantine without light exposure and close parks and beaches? It could be anything, but we do know one thing for sure: they have completely departed from the science. This is my mission to share the real science with you, for you to make your own informed decision to prevent disease.
Remember, UVB sunlight results in free radical signalling within our biologic system. These are often called reactive oxygen species (ROS). These ROS can be good and bad depending on the environmental signalling source. The antidote to the bad ROS is antioxidants. Infrared light from the sun interacting with our biology, signals the production of antioxidants. The sun is nearly 50% infrared light all the time. So, as you can see, the sun has built in a positive signalling program into its recipe. When we have full spectrum sunlight exposure on our skin and eyes, our biology is being signalled for health.

A quantum understanding of sunlight on the skin
The skin is connected to the brain quantum mechanically; they both develop from the neuroectoderm. This is evidenced in the number of Vitamin D receptors in the brain. The skin is a solar panel for the brain. Yes. You heard that correctly, you can use your skin to directly improve your brain health.
Melanin in the skin and the RPE of the eye capture highly powered photons in the UV range. This is because it is a UV fluorophore protein. When the electrons in Melanin become excited by UV radiation, these excitons are delocalised (moved), interacting with biology’s semiconductors. Some of the most important semiconductors are DHA and collagen. These delocalised excitons offload their light to excite collagen and DHA’s electrons, which acts like a flat, optimally efficient copper wire, transporting its exciton anywhere in the body it’s required. In this way, it is a perfect semi-conductor, as it moves excited electrons anywhere and everywhere, they are needed. This exciton can also be in two places at the same time. The melanin in your skin can affect your brain and can do this with no time delay at all (quantum). The implication of this is that nerve conduction doesn’t control action potentials or explain how humans think. Rather, it is the delocalised excited electrons which explain this instant communication.
The Vitamin D and Magnesium Link (Clotting, COVID and Cancer)
Blue Light, nnEMF and an indoor living lifestyle dehydrates us chronically and causes us to lose the ability to create Vitamin D and use magnesium in a proper thermodynamic way in cells. Both of these problems lead to clotting, a lack of immunity and eventually cancer. This in turn reduces the amount of melatonin the mitochondria make, impairing both autophagy and apoptosis. When this happens, disease presents because neither change program is efficient at removing defective engines/cells. This is the key reason there is a link between viral infections like COVID, clotting issues and cancer. They are all linked to a lack of sun and too much tech exposure.
A high Omega 6/Omega 3 ratio due to seed oil usage with the use of carbohydrates out of season also causes dehydration. One mole of fat creates 100-110 nmol of water. One mole of carbs produces 55 nmol of water in the mitochondria. Carbohydrates also contain more deuterium, and deuterium’s main function in the body when it gets into the mitochondrial matrix is to decrease the piezoelectric ability of the mitochondria via the increased kinetic isotope effect. Deuterium makes the mitochondria act more like a diamond, and less like quartz. A diamond’s carbon lattice is not compressible, while the SiO2 lattice of quartz is. This is why quartz is piezoelectric and why diodes aren’t. Thus, nature only creates carbs in strong light cycles when the sun can offset the lack of metabolic water production from the sun in mitochondria at cytochrome C oxidase. This is why people who eat carbs in winter start spring semester overweight.
Anyone who is struggling to get their Vitamin D levels higher likely has a co-morbid magnesium deficiency due to a lack of water from poor mitochondrial function at cytochrome C oxidase, where water is recycled/created. Magnesium and Vitamin D deficits walk together hand in hand in mitochondrial damaged patients.

NB: If you need a clotting drug, you are, BY DEFINITION already blue light toxic, nnEMF overdosed, and get far too little sun on all parts of your body.
Magnesium:
Magnesium in a cell is a hydrophilic element on the periodic table, and without water, we lose intracellular Magnesium (Mg).
56 enzymes in mitochondria use Mg2+ as a cofactor.
Making melatonin is a Magnesium and water-dependent process.
Magnesium is a co-factor for telomerase that controls our telomere lengths. This is why low Mg with a low melatonin level, cancers will come with age.
Making Vitamin D is also water and Mg dependent.
There are 3 metabolic transactions from Cholesterol (Cholecalciferol) that occur under the surface of the skin where our “storage version” of Vitamin D (Calcidiol) is made. This 25(OH) version of D3 gets transformed in our kidneys and liver to the “active version” of Vitamin D (Calcitriol or 1,2,5 (OH) in the liver. All 3 reactions require Mg2+ as a cofactor. Mg, however, needs the mitochondria to make cell water in the cell to work properly. If the mitochondria do not make water, taking an Mg supplement is a waste of time and resources. It is physiologically impossible to have a 25(OH) blood test (“Storage-D”) to be less than 35 ng/dl and a Magnesium RBC level to be above 6.5mg/dL because of the negative feedback loops tied to calcium levels in our blood!
Vitamin D’s Seasonal Addaption
Humans have been innovated by GOD or nature to live anywhere on Earth. We have built in adaption systems which allow us to generationally evolve to a completely new environment never faced before, genetically speaking. This incredible adaptive advantage has allowed us to become the dominant intelligent species on the planet. However, there are longevity advantages of seeing seasonal changes each year. If you have white skin you likely can handle the cold better than those with very dark skin. Experiencing a seasonal variation has evolved a very interesting mechanism involving vitamin D. During the summer months when UVB radiation from sunlight is abundant, Vitamin D synthesis is roaring. The body stores extra vitamin D in the form of 25 Hydroxy Vitamin D in your white adipose fat tissue. As we reach Winter, our fat stores are slowly broken down and this releases stem cells and vitamin D into our blood stream to improve our immunity. Our cells change also to promote more immune fighting cells vs growth cells. By the end of winter we have used our fat stores, are lean and fit and ready for spring to bring with it more sunlight and more carbohydrates, ready to fatten us up a little again. As Summer rolls around, this fat again stores vitamin D and stem cells and we begin the process again. This only happens if you live with nature and the seasons. Embrace nature and her cycles. If you surf her waves without a wet-suit you will likely fair quite well for a very long time.
Vitamin D and Cholesterol
CHOLESTEROL: We can’t talk about Vitamin D without talking about Cholesterol. After all, that’s what Vitamin D is made from. Did you know that?

Cholesterol is the precursor molecule for pregnenolone (precursor to Sex Steroid Hormones and Vitamin D). Cholesterol allows the intestines to absorb fat using bile. Cholesterol is in every cellular membrane giving solidity to the cell.
In fact, many of the benefits of Vitamin D3 are actually the benefits of Cholesterol Sulfate.
The only difference in both biomolecules is a single double bond in the second ring of the cholesterol backbone. This gives Vitamin D3 one less hydrogen atom than the closed ring of cholesterol.
The liver makes 85% of the cholesterol in the body. Only 15% of cholesterol comes from diet. The liver makes the very large VLDL particles. VLDL is then put into the blood and the triglycerides it contains are taken out, leading to a smaller cholesterol rich particle called LDL. The LDL then goes back to the liver within 2 weeks. In the state of diabetes, the LDL doesn’t return, and it stays in the blood longer than it is meant. This means the LDL becomes small dense LDL particles and can lead to heart disease.

If Triglycerides are high and VLDL are high, then HDL becomes worn out. High triglycerides in and of itself can destroy LDL. Increased levels of normal size LDL does not increase risk of heart disease. This type of LDL has been broken down in the blood and returned to the liver within 2 weeks. The LDL which hangs around in the blood longer than this time becomes small dense particles of LDL. This Small Dense LDL increases risk of Heart Disease by 3 times. These smaller particles can get into the blood vessel walls and form plaque. Plaque is macrophages gorging on small glycated LDL particles.
Oxidised LDL Cholesterol can cause arterial issues: The oxLDL came from LDL cholesterol made in the liver that spent too much time circulating in oxidized plasma. The main reason for this is poor endocytosis in the portal circulation and/or poor LDL receptor function causing it’s slow uptake by your cells. oxLDL depletes the arteries of K2, requiring an additional supplement from diet.

Large LDL particles are good. Small LDL particles are dangerous. Statins scavenge sdLDL, this is why they work. This is why it’s wise to limit or eliminate processed foods or triglyceride latent carbohydrates as much as possible.
Sunlight lowers cholesterol
When the skin produces cholesterol sulfate, your blood cells becomes sulfated, and this helps augment the DHA fatty acids in the Red Blood Cells (RBC) to generate a net negative charge to repel the net negative charge in Exclusion Zone (EZ) water in the blood plasma. This improves the flow, by improving laminar flow, and it increases the motion of blood in the arterioles and capillaries of the skin by proton motions caused by UV and IR light in the sun. The blue light and UVA light act in unison to vasodilate blood vessels in the skin in different ways. Blue light uses melanopsin to do this, while UVA light uses nitric oxide (NO). The reason this is done is to create an electric and magnetic field within the blood vessel to activate NO production from the glycocalyx of the arteriole wall and the arterial wall in a controlled fashion. The quanta of light control this process. These actions all work in concert to allow massive amounts of cholesterol to be bound to sulfate. This makes cholesterol water soluble. When this occurs, cholesterol does not have to be tightly bound to LDL particles made from the liver. As a result, LDL cholesterol drops.
Non-native electromagnetic fields (nnEMF) destroy cholesterol in the skin. This reduces the body’s ability to convert sulfate cholesterol to Vitamin D.
Sulfated Vitamin D3 acts as a natural calcium channel blocker in the skin. Calcium channel blockers act to lower blood pressure by increasing proton flows in blood vessels.
When calcium levels are altered in the CSF and the blood, cholesterol in the basal skin and blood plasma cannot be sulphated from cysteine stores. The cysteine stores use vitamin B12 which fits perfectly with nNOS hydrophilic hems pocket. It then binds some glutathione from the RBC in the plasma. Glutathione has the ability to carry an extra sulfur atom in the form of GSSH.
Skin is a giant solar powered battery to make sulfated proteins in its arterioles. In many ways, this sulfated version of cholesterol and Vitamin D3 perform the same functions of chlorophyll in plants. These proteins are designed to diffuse sunlight and help you retain water while absorbing on the specific wavelengths of light that cholesterol and Vitamin D need to keep you well. When you do not get those frequencies all quantum hell breaks loose because of calcium efflux.
Calcium efflux is the key metric to the change in the metabolic sensor in seasons. The SCN goes from its light switch (summer) to its cold switch (winter).
In Summer, we use eNOS with the photons of UVB and IR light to make sulfated proteins to deliver cholesterol and oxygen to tissues that need it.
In Winter, we use eNOS to deliver cholesterol and oxygen to tissues that need it using a plasma that is more loaded with electrons.
When the cell experiences calcium e-flux for any reason, (non-native EMF #1 cause today), cells immediately switch from making sulphate in surface blood vessels to nitrate synthesis. So, sulphate levels drop everywhere. This directly affects Vitamin D 3 and cholesterol function. Neither can be sulphated as they normally would be, even when the sun is shining brightly. With exposure to nnEMF, the body cannot make sulphate in the skin when the sun hits it. This is why dermatologists believe the sun is bad. Solution: Remove the nnEMF and sun is good!
Homocysteine is the source of sulphate. Sulphate comes from homocysteine recycling that occurs within RBC’s haemoglobin in the surface arterioles in our skin. RBC’s supply the ATP to the plaque so that sulphate can be produced from homocysteine. ATP withdraws electrons from homocysteine to sulphate the cholesterol in blood. The body needs some endogenous glucose production in RBC’s to make small amounts of ATP to move electrons. It does this via anaerobic conversion of glucose by the Embden-Meyerhof pathway for the generation and storage of high-energy phosphates. Sulphate stores in the body can be regenerated fastest by eating seafood and pork!
Cholesterol depletion in cell membranes forces cells to switch to nitrogen based O2 transport. Normally, this only occurs in the absence of sunlight in Winter. In our modern environment, it happens 24/7 while people eat a carbohydrate rich diet…
Cholesterol sulphate is manufactured by a combination of specific frequencies of
Ultraviolet Radiation (UV)
Visible Light Radiation (VL)
Infrared Radiation (IR)
and a specific range of oxygen saturation in our blood


Interesting Vitamin D facts:

An increasing Vitamin D OH-25 is linked to a reduction in all-cause mortality. http://ar.iiarjournals.org/content/38/2/1173.full
The lower your Vitamin D, the less pain you can tolerate.
The more obese the individual is, the more Vitamin D they need to sustain their immune system.
80 different metabolic processes are improved by improving Vitamin D generation.
Serotonin levels may increase in the brain when Vitamin D increases
Sunlight is a Calcium Channel Blocker & lowers Blood Pressure. Sunlight is a natural calcium channel blocker in the skin. Calcium channel blockers act to lower Blood Pressure by increasing proton flows (enzyme function) in blood vessels. Blue light and other nnEMF interfere with calcium homeostasis in the cell. Blue Light and other nnEMF (including 5G) raise Blood Pressure and may lead to clotting.
Vitamin A toxicity can be completely avoided with a high Vitamin D. Seafood is even good in low light cycles, as long as its eaten with nature.
Diabetics generally have low Vitamin D. All cancer patients have low Vitamin D. Anyone with an autoimmune condition has low Vitamin D.
Vitamin D has profound activity as an antioxidant as well as it's mineral absorptive and other benefits.
When the mitochondria are not working as well there is less energy availability to sulfate cholesterol to create Vitamin D upon UVB light exposure.
Non-native electromagnetic fields (nnEMF) destroys Vitamin D. When nnEMF is present, it causes oscillations. These oscillations knock electrons off cell membranes, and once these electrons are knocked off, we are unable to make Vitamin D effectively from UV light.
At 75 years of age, your ability to generate Vitamin D from your skin is diminished by 75%. However, you can still generate it.
If living in a strong solar environment this will help mitigate the higher inflammatory diet of fructose and carbohydrates because it raises Vitamin D, T3, LDL, DHEA and Melatonin.
Vitamin D regulates the elasticity of blood vessels and thus also affects blood pressure amplitude. Vitamin D relaxes blood vessels. The results were published earlier this year in the journal Molecular Endocrinology.
Allergies are usually associated with a low level of Vitamin D
“Vitamin D3 remains in the skin even when the skin is washed with soap.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3897598/?fbclid=IwAR2zr9aCpQ5hvIhI41bf-LA3CP8Lm_67QWqTZl-pSLmce-mj0Cfp_F66pjc
Intracellular hydration is critical for Vitamin D synthesis. The sun is how we build our redox potential through water. When you are born you are 80% water. When you are 60 you’re about 60% water. Remember, we make water in our mitochondria and peroxisomes within every cell. It is estimated by Lazlo Boros that our cells collectively recycle upwards of 3,000 litres of water per day. So, losing water concentration in our body as we age is akin to our mitochondria not working as well as they did to recycle water as when we were young. The key way we enhance this recycling efficiency is through sunlight exposure. As we get older it becomes more important to be out in the sun because our mitochondria do not make as much matrix water given Heteroplasmy increases with age. This also implies that when unwell, water becomes more important to drink water. The sun helps the hydrogen bonding network in water.
The more you smoke the more sun you need. Tobacco inhalation will damage your mitochondria, however, the more sun you get the less mitochondrial damage you will create. Here’s a meta-analysis on Vitamin D and smoking. https://pubmed.ncbi.nlm.nih.gov/34646549/
What does Vitamin D do and what should you know about Vitamin D?
Facilitates increased intestinal absorption of phosphorus and calcium as well as suppression of parathyroid hormone secretion to increase our plasma calcium concentrations. It, however, does not dictate or direct where this calcium will be deposited in our bodies. Note: there is also not a strong negative feedback control loop within the gut for Vitamin D.
Avoid insulin resistance, weight gain and T2D. Levels above 50 ng/ml are associated with increased adiponectin levels and low leptin levels. High adiponectin and low leptin levels means you are less likely to be obese. So higher vitamin D levels can help us trim our fat stores and offset the effect of seasonal carbohydrates in causing weight gain. By decreasing fat levels, we can avoid the initial steps that lead to insulin resistance and avoid eventually developing Type 2 Diabetes.
Vitamin D powers the immune system via T cells, WBC’s and inflammatory pathways (nFKB & TNFa). Vit D is a natural antibiotic that assists WBCs in clearing infections. It does this by stimulating immune cells to make a protein called cathelicidin in our skin. This does not happen well in our gut, but works like a charm in our skin with UV and IR exposure. This protein is found on T cells within our skin, macrophages, neutrophils, and on our epithelial cells in our guts and respiratory system. It actually helps defend us from viruses and bacteria all the time when its optimized. In our gut linings, it also activates the T regulator cells to protect the intestinal lining and the GALT that lies right behind the brush border. The light required for this activation may come from the prokaryotes in our gut microbiome who naturally release large amounts of light. Our enterocytes have to contain DHA in their cell membranes to decipher the signal properly. It now appears that low vitamin D status in the gut may be a huge risk factor for the development of HIV general infection. Another major immune effect of Vitamin D is that it has the ability to block intracellular signals of NF Kappa beta and of TNF alpha. Both of these chemicals are part of the machinery that causes up-regulation of the stressful cellular response mechanisms in many pathologic diseases like cancer, autoimmunity and in obesity.
Boosts kidney health. It’s a direct inhibitor of the hormone renin in our kidneys and helps protect us from developing systemic systolic blood pressure elevation. It also protects the kidney directly from high levels of uric acid production that come from end stage fructose metabolism.
Vitamin D protects against heart disease (higher HDL). When you optimize your vitamin D3 with sunlight, you will notice your HDL will rise 10-30% in the first year. I look at low HDL as a cause of low redox and poor solar exposure. This signifies that the liver is doing a better job of “skimming” the portal circulation for endotoxins. This is the major mechanism by which Vitamin D protects the heart, in my view. We all hear from doctors that a high HDL protects the heart. This is how: It makes the liver a master of defence for the nervous system. It also protects the brain from endotoxin assault from the gut, it reduces all causes of mental illness and it is a main defence in the brain gut axis. Higher levels of VDR activation means less hypoxia in the brain and better mitochondrial density and function in the brain and heart. This increases the magnetic sense within mitochondria by increasing electron tunnelling on the inner mitochondrial membrane. Furthermore, a single nucleotide polymorphism (SNP) has been linked to the development of early heart disease. This SNP is on the C allele of SNP # rs4646536 and is being studied in the NIH VITAL trial currently ongoing. This is a second mechanism to prevent heart disease.
Improves skin health. When the skin makes Vitamin D3 naturally, usually 10-20,000 IU are made locally in the skin. The excess Vitamin D3 is then broken down to its degradation products, which have been shown to inhibit the development of psoriasis in studies. These degradation products prevent the proliferation of the lower levels of the skin from reproducing at a faster rate than normal. This is the pathology found in psoriasis. The lower epidermis is known to grow 25-40 times faster and the skin gets a large red plaque on its surface as a result. This is why light therapy is so effective in treating psoriasis. It’s kind of ironic that dermatologists don’t look at the pathological causes of this disease. Here, sunlight is curative because it stimulates Vitamin D3 production to make excess Vitamin D3 to make degradation products. Anyone with psoriasis should have their Vitamin D levels checked and optimised before they do anything else. Most have extremely low levels and they tend to be obese and have higher cancer rates across the board.
Vitamin D helps prevent and reverse autoimmune disease (AI). In autoimmune diseases, we need to advocate for much higher levels of Vitamin D from sunshine. Those with AI have poor gut function due to an altered microbiome. They also tend to be DHA depleted. In order for circulating vitamin D to perform its functions, it must first activate the vitamin D receptor (VDR). Many people with autoimmune disease have a genetic polymorphism that affects the expression and activation of the VDR and thus, reduces the biologic activity of vitamin D within the skin and gut. Studies have shown that a significant number of patients with autoimmune diseases have several VDR polymorphisms. There are over 25 variants of VDR polymorphisms now known and the list grows monthly. If you have a VDR problem, you require much higher circulating levels of Vitamin D from sunlight to bind to these defective receptors. A leaky gut predisposes to the development of autoimmunity. Fundamentally, the leaky gut may be due to a lack of bacteria leaking UV and IR light to our enterocytes to activate the innate immune system and the VDR. Moreover, optimal Vitamin D levels are also linked to “tighter junctions” between the enterocytes of our intestinal lining making our guts “less leaky.” If the gut is less leaky, our immune system is stronger because it does not have to be activated constantly to protect the rest of the body. We have also seen above that vitamin D levels play a huge role in our immune surveillance in our GI tracts. It appears to be critical to push your levels to much higher plasma levels in these cases. I strongly recommend talking this over with your doctor. The fears of Vitamin toxicity from sunlight are very overblown in my estimation and the risk of too low a level for disease propagation is far too common and risky for your health. There is a concern about oral vitamin D supplementation in case where non-native EMF predominates. There is now very recent evidence out from Dr. Hector DeLuca about MS and autoimmune encephalitis. Dr. DeLuca believes that the degradation products of vitamin D3 and/or some by-products of solar radiation confer health to us in some fashion. He says vitamin D3 degradation and sunlight is somehow active against a range of autoimmune illnesses. In his latest work, that “something” he is studying is active against an experimental model of multiple sclerosis. I have always felt that MS, ALS and Guillian Barre are tied in some fashion to vitamin D metabolism and a loss of light. It appears Dr. DeLuca believes this as well.
Vit D is fat soluble and requires good gut health for optimal absorption. If eating Vitamin D, eat it with fat (i.e. seafood). Vitamin D is a fat soluble molecule. It means it should be taken/eaten with fat for absorption, hence why it’s in seafood. But it also means that those with a leaky gut, IBD, Crohn’s, Ulcerative colitis, liver disease, those without a gallbladder, and those on a low-fat diet that 99% of nutritionists and dietitians recommend will not absorb well either. Furthermore, if you are on NSAIDs, steroids longer than two weeks, blood thinners or anticoagulants, reflux medicines and antacids, and synthetic hormones like birth control pills, you also won’t absorb Vitamin D well at all. Are you starting to understand now why we have an epidemic of hypo vitaminosis of vitamin D?
Hypothyroid/Hashimoto’s Disease can signify poor Vit D function despite a high level of Vitamin D in the blood. 90% of hypothyroidism in Australia is a result of Hashimoto’s disease. This disease is an autoimmune disease and these patients universally have defective VDR receptors. That means they need very high levels of blood Vitamin D levels from sunlight and optimization of their thyroid function to get results. Often, many obese people get stuck not losing weight because their doctors are fooled into thinking their thyroid and Vitamin D levels are fine. Most of the time, the levels are sub-therapeutic and patients find amazing results when their plasma levels are pushed a bit by the clinician. The problem is most MD’s are afraid to advocate for the sun’s light. Post op cancer patients and high cortisol individuals also often have this issue.
High Vitamin D keeps your mitochondrial heteroplasmy low and your skin anti-aged. Age will decrease your skin’s ability to make Vitamin D3 from sunlight and cholesterol. As we go from age 20 to 60, we lose that ability by a four-fold magnitude. The darker our skin, the worse the conversion. So, as we age, we need more sun or supplementation, not less of either. This is why so many older people see a higher incidence of neolithic diseases as well.
Eat Epi-Paleo to make Vitamin D Binding Protein (DBP). This will allow you to make more Vitamin D than you need to fill your savings account. Humans have a Vitamin D savings bank in our body. It is supported by a good protein diet and leads to a better Vitamin D level. An Epi-paleo diet is an optimal choice for this bank account. It works by making a protein called Vitamin D binding protein (DBP). It acts like albumin does in the blood. The vitamin D-binding protein (DBP) is a highly specific carrier for vitamin D and all of its metabolites found in the plasma. This allows us to store vast amounts of Vitamin D. Vitamin D synthesis from cholesterol by the sunlight is thus maintained within physiological limits estimated to be 0.01 to 2.5 mg of cholecalciferol per day. 2.5 mg per day translates to 100,000 IU per day! If we are protein deficient, we do not have this ability and our stores are low, in low light levels. It not only protects our Vitamin D stores, but it also prevents the toxic effects of a high vitamin D level in the blood. Humans start to store Vitamin D3 when Vitamin 25(OH)D level is above 40 ng/ml. The interesting finding is that it is only around a level of 60 ng/ml that the stores are sufficient to see us through a winter with a resultant optimal D level. This is why dietary composition is critical for immunity the further one gets from the equator. Seafood is on of the few foods high in Vitamin D levels. At the equator there are no foods with Vitamin D because the tropical sun provides all we need. This information also shows why flu season peaks in winter months in epidemiological studies. It also helps explain why those who are chronically ill or have serious diseases like cancer have very weakened immune systems. This is why cancer patients have higher risks for developing multiple neolithic diseases as they age. Peripheral neuropathy and pain is one such example. Those with low HDL levels or frank liver disease tend to make the lowest amounts of DBP. The liver is our organ that really is a solar organ that mimics photosynthesis. Liver disease or low HDL states are seen in hepatitis cases and in patients with metabolic syndrome as well. It also explains why other neolithic diseases afflict those people and why they all seemingly have low vitamin D levels, too. This is why we see an epidemic in Australia today. Before, we never looked for it, but now we are beginning to understand just how vital Vitamin D is for immunity and health.
High Vitamin D = Anti-aging Telomeres. In 2007, Richards found that higher vitamin D levels are also associated with longer telomere lengths. This means that optimal vitamin D levels reduce our cellular aging risk, reduce utilization of our stem cells, and decrease the leakiness of our mitochondria which drive the action of the telomerase enzyme that dictates telomere length. So it makes sense if your D level is low, your telomeres will be shortened and this, too, will put you at heightened risk for neolithic disease. All cellular systems seem to point to disease and increased aging with lower vitamin D levels. Aging is also associated with calcium efflux in mitochondria. This is among one of the most congruent findings I have seen in biology since I began to review the biochemistry and literature in this area.
A bad/toxic environment triggering Hypermethylation can override Vitamin D3’s anti-cancer benefits. The gene that codes for E-cadherin can be epigenetically silenced via promoter hypermethylation. This explains why Vitamin D3 cannot “prevent” or “cure” all cancers, since the E-caherin gene is under the direct regulation of Vitamin D3. Hypermethylation is the on/off switch with regards to cancer. Solution: Stop the hypermethylation and boost Vitamin D3.
Vitamin D improves athletic performance. Want proof? Just ask the team that just won the Grand Final, Superbowl, Olympics, Stanley Cup or any other major event. I bet they have coaches monitoring and maintaining their Vitamin D levels.
Vitamin D may lower Breast Cancer Risk. It is also vitally important to our immunity and defence. New studies in 2009 showed that that Vitamin D also decreases the risk of breast cancer in women when their levels were over 50 ng/ml (125 nmol/L). The ApoE4 allele is the allele that conferred the ability of humans to leave Africa and evolve and live in environments with lower levels of solar radiation, yet still capture enough Vitamin D to survive. This allele is associated with other diseases these days, but it was ideally matched for humans who needed to migrate north and south from the equator for many reasons.
Have you tested your Vitamin D level lately?
If you go to your local GP or Primary Care Provider and request a 25 Hydroxy Vitamin D + a 1_25 Hydroxy Vitamin D test + a parathyroid hormone test, you will be well on your way to uncovering the state of your immune system and redox power. Once you have the results you can reach out to me for interpretation if via a coaching session here if you’d like.
Trending VD1_25 labs tell you about an acute change in your environment likened to inflammation.
Testing VD25(OH) is like a bank account as it is more accurate over a long time.
Testing Parathyroid Hormone (PTH) along with the above will give you an indication of your bone health, mineral balance, and calcium status.
Unsupplemented Vitamin D levels are great proxies for defects in Vitamin A cycles in the brain and retina.
I hope you discuss this information with your doctor and decide on a new healthy course. Your health depends upon it.
I’m on a mission to stop myself from going fully blind. I’m using my skin to do this. I’m writing a book about my health journey. It’s almost done, and I can’t wait to get it to you!
If you enjoyed this blog and would like to support me, you can donate here to help me publish the book.
Stay golden, tanned, healthy and happy!
Nathan
Citations and references:
Vitamin D Meta-Analysis: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4103214/?fbclid=IwAR2zIeBwaWbogKyvNXr2MYDXGv12UrSAN_cjZuUF7fIqYr7NMp8KRP6Pzmg
A void Supplementing Vitamin D unless you know what you are doing. https://myersdetox.com/103-rethinking-vitamin-d-toxicity-with-morley-robbins/
Alexander Wunsch – Vitamin D and COVID-19 https://www.youtube.com/watch?app=desktop&v=2UANAzTYGgI
Cholesterol and Vitamin D are very similar https://people.csail.mit.edu/seneff/London2014/SeneffHeartDisease2014.pdf`
Understanding cholesterol https://www.youtube.com/watch?v=OyzPEii-wo0&t=4s
Vitamin D and The Immune System – https://link.springer.com/chapter/10.1007/5584_2018_246 and https://www.sciencedaily.com/releases/2010/03/100307215534.htm
Vitamin D from food – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2665033/
25-Hydroxylation of vitamin D3: relation to circulating vitamin D3 under various input conditions https://pubmed.ncbi.nlm.nih.gov/18541563/
Summary of roundtable discussion on vitamin D research needs https://pubmed.ncbi.nlm.nih.gov/18689407/
Is Vitamin D Deficency a Major Global Health Problem https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4018438/?fbclid=IwAR2Flz-TBwlaXcWmlXLYeJg31kXo93pA6OcsWGK42kqScY4CmVx4uplCtoc
Seasonal Variation in Vitamin D – https://www.wired.com/2015/05/dna-changes-seasons-just-like-weather/
Vitamin D and Smoking Meta-Analysis https://pubmed.ncbi.nlm.nih.gov/34646549/
Otten JJ, Hellwig JP, Meyers LD. Vitamin D. In: Dietary Reference Intakes: The Essential Guide to Nutrient Requirements. Washington, DC: National Academies Press, 2006.
Institute of Medicine Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
Thorne J, Campbell MJ. The vitamin D receptor in cancer. Proceedings of the Nutrition Society. 2008;67(2):115-127. [PubMed Abstract]
Moreno J, Krishnan AV, Feldman D. Molecular mechanisms mediating the antiproliferative effects of vitamin D in prostate cancer. Journal of Steroid Biochemistry and Molecular Biology 2005; 97(1–2):31–36. [PubMed Abstract]
Holt PR, Arber N, Halmos B, et al. Colonic epithelial cell proliferation decreases with increasing levels of serum 25-hydroxy vitamin D. Cancer Epidemiology, Biomarkers, and Prevention 2002; 11(1):113–119. [PubMed Abstract]
Deeb KK, Trump DL, Johnson CS. Vitamin D signalling pathways in cancer: potential for anticancer therapeutics. Nature Reviews Cancer. 2007;7(9):684-700. [PubMed Abstract]
Ma Y, Zhang P, Wang F, et al. Association between vitamin D and risk of colorectal cancer: a systematic review of prospective studies. Journal of Clinical Oncology. 2011;29(28):3775-3782. [PubMed Abstract]
Gandini S, Boniol M, Haukka J, et al. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. International Journal of Cancer.2011;128(6):1414-1424. [PubMed Abstract]
Woolcott CG, Wilkens LR, Nomura AM, et al. Plasma 25-hydroxyvitamin D levels and the risk of colorectal cancer: the multiethnic cohort study. Cancer Epidemiology, Biomarkers & Prevention. 2010;19(1):130-134. [PubMed Abstract]
Jenab M, Bueno-de-Mesquita HB, Ferrari P, et al. Association between pre-diagnostic circulating vitamin D concentration and risk of colorectal cancer in European populations:a nested case-control study. BMJ.2010;340:b5500. [PubMed Abstract]
Wactawski-Wende J, Kotchen JM, Anderson GL, et al. Calcium plus vitamin D supplementation and the risk of colorectal cancer. New England Journal of Medicine 2006; 354(7):684–696. [PubMed Abstract]
Chung M, Lee J, Terasawa T, et al. Vitamin D with or without calcium supplementation for prevention of cancer and fractures: an updated meta-analysis for the U.S. Preventive Services Task Force. Annals of Internal Medicine. 2011;155(12):827-838. [PubMed Abstract]
IARC Working Group on Vitamin D. Vitamin D and cancer: A report of the IARC Working Group on Vitamin D. IARC Working Group Reports. Lyon, France: International Agency for Research on Cancer, 2008.
Yetley EA, Brulé D, Cheney MC, et al. Dietary Reference Intakes for vitamin D: Justification for a review of the 1997 values. American Journal of Clinical Nutrition 2009; 89(3):719–727. [PubMed Abstract]
Manson JE, Bassuk SS, Lee IM, et al. The VITamin D and OmegA-3 TriaL (VITAL): rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemporary Clinical Trials. 2012;33(1):159-171. [PubMed Abstract]
Pereira F, Larriba MJ, Muñoz A. Vitamin D and colon cancer. Endocrine-Related Cancer. 2012;19(3):R51-71. [PubMed Abstract]
Wu S, Liao AP, Xia Y, Li YC, Li JD, Sartor RB, Sun J: Vitamin D Receptor Negatively Regulates Bacterial-Stimulated NF-{kappa}B Activity in Intestine. Am J Pathol. 2010 Jun 21
http://www.webmd.com/breast-cancer/news/20110429/low-vitamin-d-linked-to-aggressive-breast-cancer
www.vitamindcouncil.org/health-conditions/cancer/breast-cancer/
www.ncbi.nlm.nih.gov/pubmed/21278761
www.ncbi.nlm.nih.gov/pubmed/19346976
http://rstb.royalsocietypublishing.org/content/365/1554/2835.full
http://www.ncbi.nlm.nih.gov/pubmed/19307527
http://www.ncbi.nlm.nih.gov/pubmed/20308557)
http://www.lmreview.com/articles/view/vitamin-d-and-vitamin-k-team-up-to-lower-cvd-risk-part-II/
http://www.ncbi.nlm.nih.gov/pubmed/6299329 Fiber depletes Vitamin D levels.