
The Global Experiment #3 - Natural Immunity and Adverse Reactions
Today’s blog will cover:
Ideas to create a more human future filled with family, love and freedom.
Vaccine Adverse Reactions and Symptoms
The new Pfizer vaccine approved by FDA
MTHFR C677T, Homocysteine and their link to Thrombosis risk from vaccination.
Employer, school and university mandates of COVID vaccination and how to counter it.
The pseudoscience of ‘Long COVID’.
How you can cultivate Innate Natural Immunity
Take a look at the citations, lots of great ones in there.
As always, here’s the note about viruses that we always begin with in this series. Viruses are how we make new genes. Nature has told us that viruses are good. We are designed to assimilate them. Human DNA is made of 98% HERV-1 retroviruses. Viruses are not bad. Ok, let’s begin!
It’s October 2021 and we find ourselves in a predicament. The science is emerging that these injections may not be the best way to deal with the so called ‘pandemic’. So why is the experiment continuing? You may engage in high octane speculation, but in my view the agenda has not changed.
A digital control grid is being created. Fuelled by mass toxification of our food, water, medicines, homes, workplaces, skies, cities and electromagnetic environment. But why? My guess is to save the governments, banks and insurance companies trillions of dollars whilst securing more control over populations. Digital identities, health in a pill, not needing to work by being on a universal basic income (UBI), entertainment on demand, space travel, clean free energy, digital financial systems and autonomous transport are all realities if we fund and work to build them. But there is a cost to all of this. You begin to lose yourself in a low vibrational reality fuelled by consumerism and a lack of independent thinking, not to mention a decline in health. This reality painted by Zuckerberg, Musk, Carsterns, Powell, Morrison, Bezos, Cook, Gates, Rockefeller, Rothchild and all their friends cannot be created if you begin at the community level, building a multidimensional human future. How? Connect to nature around you, spend quality time with friends outdoors, detox from technology and plug into observational wisdom. Play, laugh, dance, adventure and give your gift every day to those around you. Live a Foundational Health Lifestyle and your energy will be abundant. What was your favorite thing to do when you were 8? Do that. Connect with animals, paint and sing, write and read a book, learn a new skill or trade, learn how to grow a veggie garden or look after chickens. The possibilities are endless. At the same time work towards becoming financially independent. Lower your living expenses, adopt a DIY (do it yourself) attitude, get an extra rain water tank, rent out one of your rooms to a trusted tenant, carpool with other healthy people and start a community initiative with your tribe.

This week my friend and I started a Beach Buddies Bespoke Breakfast initiative raising awareness for a healthy lifestyle. You can find us on the main beach in Agnes water, Queensland, Australia every second Sunday where we bring tables and chairs to the beach and discuss only the most important topics over a high fat and protein breakfast at sunrise.
What will be your expression of how to create the world you want to live in, instead of going along with someone else’s narrative?
Let’s begin. The experiment continues… hop on board and let me take you on a journey over the past few months as it relates to you and your family’s health.
Back in July, Dr. Robert Malone, the pro-vax inventor of using mRNA as a drug, shared with us that vaccine adverse events reporting system (VAERS) under reports adverse events by ~100 fold. So, every time you read or hear about an adverse event, such as a death post vaccination, there is another 99 who experienced the same thing, but did not find the time to report the event. If you haven’t listened to his talk, it’s probably the most important podcast to understand the issues around mRNA therapies. mRNA is a drug, and the altered spike protein is a toxin to cells. This has big implications. https://www.youtube.com/watch?v=nYkUePQMfkE&t=1s
So, who is at risk of death from COVID-19? Age is a metric commonly used, the older you are the higher your probability of a poor outcome. However, the CDC completed a study for us showing some surprising conclusions about high-risk categories of poor COVID-19 outcomes. The study concluded, "Among 4,899,447 hospitalized adults in PHD-SR, 540,667 (11.0%) were patients with COVID-19, of whom 94.9% had at least 1 underlying medical condition. Essential hypertension (50.4%), disorders of lipid metabolism (49.4%), and obesity (33.0%) were the most common."

"The strongest risk factors for death were:
Obesity (adjusted risk ratio [aRR] = 1.30; 95% CI, 1.27–1.33)
Anxiety and fear-related disorders (aRR = 1.28; 95% CI, 1.25–1.31)
Diabetes with complication (aRR = 1.26; 95% CI, 1.24–1.28)
As well as the total number of conditions, with aRRs of death ranging from 1.53 (95% CI, 1.41–1.67) for patients with 1 condition to 3.82 (95% CI, 3.45–4.23) for patients with more than 10 conditions (compared with patients with no conditions)."
Study: https://www.cdc.gov/pcd/issues/2021/21_0123.htm
What about all these lockdowns, mandates, and restrictions? Are they being used in part to hasten the economic reset? Yep.
Dr. Tess Lawrie founded the Evidence-Based Medicine Consultancy Ltd, a specialist firm committed to improving the quality of healthcare through rigorous research. She explained in a recent interview with UK’s Paul Graig Roberts: “I haven’t seen any good evidence that lockdowns or masks work. More concerning, we’ve known that ivermectin works for some time, and doctors have been trying to communicate this message to the authorities, who have been very single-minded in their strategy and approach. If ivermectin had been employed last year, when the UK authorities were notified, there would have been no lockdown in my opinion.”
Many of the COVID policies appear suspiciously about something other than a virus. Many policies directly relate to an economic reset. One of these motivations appears to be saving the pension funds huge sums of money by reducing the life expectancy of many, especially the elderly and making money whilst doing so. Money grabs are everywhere.; the amount of excessive fiscal stimulus, creating money out of thin air with quantitative easing and using the taxpayer’s assets and income as collateral. That’s all of us. This is not a downturn of the economy, it’s an economic take-down. What is in the injections? Why were they rushed out for a disease with such a high survival rate? Why were messages about boosting your immune system with Vitamin D, zinc, quercetin, and vitamin C not widely shared on mainstream news channels? Why was a hydroxychloroquine manufacturing plant destroyed in Mexico by a random fire? Why has Ivermectin use for COVID-19 been banned in so many countries when India just declared their most populated state COVID free citing widespread Ivermectin use? Why have many countries jumped on the injection bandwagon without short, medium, or long-term phase 1, 2 and 3 clinical trials of safety and efficacy? Why has Moderna’s COVID-19 vaccine been so successful, pulling Bill Gates’ company from bankruptcy to outperforming the S&P500 since the beginning of 2020? Meanwhile, why has Bill Gates become the largest farmland owner in the USA? And why are we injecting children, who have strong innate immune systems, with an experimental gene therapy when they are at almost no risk of death from COVID-19? Why are healthcare workers quitting their jobs in protest based on vaccine mandates? What do they know that we don’t? All these questions and more point towards a non-health agenda…

On September 13th, Moderna submitted data on boosters. The FDA was evaluating data on Pfizer boosters. Israel was about to send their data on boosters to the FDA. Yet the administration announced that boosters will be available Sept 20th. Is that policy informing science or science informing policy?
It is political science trumping biological science. We're being ruled by fools. COVID appears to be a compliance test for an economic war on the taxpayer.
Back to the science.
Why the VACCINES and BOOSTER shots DON'T and WON'T work:
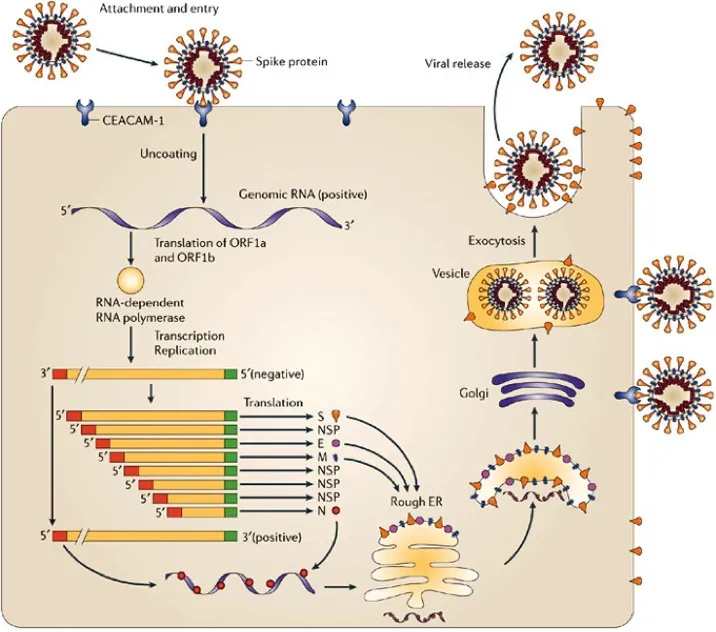
The SARS-COV2 virus has a large number of surface features called “antigens.” There are four major ones: the spike (S), envelope (E), membrane (M), and nucleocapsid (N). When a person is exposed to SARS-COV2, the virus enters cells, hijacks cellular machinery, and replicates itself, allowing the process to repeat itself.
Once a person is exposed to the virus, the immune system develops antibodies to the S, E, M, and N antigens. T-cells are keyed to all of them as well. Because immunity from infection develops to all four antigens, it is much more robust and longer lasting than the shots.
Since COVID-19 is thought to be a serious threat, it should be beneficial to short circuit the process by introducing antigens to create immunity without causing the disease or side effects. Indeed, a perfect vaccine would do this. For example, the polio vaccine is close, and uses “crippled” viruses in a way that should prevent the disease, but even it still causes about three cases of polio per million doses given.
The Johnson and Johnson COVID-19 vaccine is relatively traditional. It uses a crippled adenovirus that has the Alpha variant S antigen added. The Pfizer and Moderna products are different. They use the patient’s own cellular machinery to make the Alpha S antigen by injecting messenger RNA. So all three vaccines ultimately produce only the Alpha Spike protein antigen. Your immune system then creates T-cell and antibody immunity to just the Alpha Spike protein. They don’t confer immunity to any of the other three antigens.

This creates a serious problem on two fronts.
First, because the shot gives immunity to the Spike protein of the Alpha variant of COVID-19, it does a pretty good job of shutting down the Alpha variant. But viruses are constantly mutating. Just think of how many strains of flu there are. Each year we get a new set, and vaccine makers have to guess at which ones to mix in this year’s cocktail. When the vaccine shut down a lot of the Alpha variant, other variants got through and multiplied. This is the superbug problem. The Delta variant popped up in India and soon spread around the world. Now we have Lambda and Mu variants showing up. Their largest difference from Alpha is in the spike protein. By killing off the Alpha variant, only mutations that are less well controlled by Alpha Spike immunity survive. It’s the exact problem with overuse of antibiotics. There, only the bacteria that aren’t affected by the antibiotics are left. Here, only the variants that aren’t beaten by the shot survive. With COVID-19, if the other three antigens were included in the vaccine, we’d have robust immunity, and no boosters would be required, since the shot would produce roughly the same response as an illness would. Instead, we are seeing new illnesses arise that are less and less responsive to the current vaccines on offer. But the booster that’s being promoted is only for the Alpha Spike protein, and thus is doomed to be poorly effective against new variants.
The second problem is proving to be far more serious. The shot was (and is still being) promoted as very safe, with minimal side effects. This is, unfortunately, false. I won’t go into the litany of deaths and severe disabilities that come from the vaccine. Those are well documented (here, here, and here). For our purposes, we need to understand one simple fact. The Spike protein is the disease causing agent in COVID-19. It causes inflammation in blood vessels leading to clots, and that inflammation later on causes the “cytokine storm” that kills people. We can visualize the progress of the disease like this.
Early on, while the Spike protein is doing it’s dirt, there’s lots of virus around. That’s when we get immediate deaths, clots causing strokes, myocarditis in young men, and all those other bad things. It’s only later on, when the virus is already gone, that the patient’s immune system goes completely haywire (cytokine storm) and more harmful effects like ADE appear.
All of these side effects could be completely avoided by making a vaccine using a different viral protein (or three) that stimulates immunity. But the Alpha Spike protein that the vaccine uses is the problem. In short, the current vaccination program is actually giving people a case of COVID. Because it doesn’t continue replicating like a live virus, it’s usually short and mild, but in some people it’s deadly. And it can’t produce the long-lasting robust immunity that exposure to all four antigens creates.

Why does being vaccinated make you a ‘Super Spreader’ of the virus?
Another key feature of the vaccines is that they are humoral (blood) immunity to an airborne virus.
COVID-19 viruses enter the body through the air sacs (alveoli) in the lungs. There they encounter the pneumocytes, attach to their ACE2 receptors and get inside. They multiply, and release lots more viruses. Most of those new viruses will go back into the alveoli, where they can be breathed out to infect someone else.
This happens before any viruses get into the bloodstream (red arrows) to encounter antibodies and killer T-cells. That means that an immunized person can still get infected and shed enough virus to infect someone else. Vaccines can’t stop that. Notice I didn’t say “won’t.” I said “can’t,” as in, “there’s no possibility.”
It’s only after viruses are released across the alveolar basement membrane into the bloodstream that antibodies and killer T-cells can get to work. If you’re immune, then the viruses will get wiped up quickly and you won’t get sick. But you still got infected. And you can share it with someone else. The vaccine won’t ever change that.
There are huge problems with the vaccine program as currently promoted.
First, instead of being low risk, it’s the highest risk that could possibly be engineered, since it’s based on giving you the active disease causing agent.
Second, it cannot prevent you from getting infected and passing the disease on to someone else.
Third, the use of the vaccine is literally causing variants that vaccine immunity is less effective against to emerge.
Fourth, the booster regimen is targeted against a Spike protein that isn’t around much anymore. And it predisposes to something bad called Antibody Dependent Enhancement.
In short, the entire Spike protein based vaccination program is bad medicine. It is making us sick. We need a different vaccine without it. (Or none at all.) And until that arrives, we need ready access to drugs to treat COVID-19 at home, before that cytokine storm puts one of our feet on the banana peel.
In Australia, Pfizer and Moderna have already re-branded their injections... Why do companies re brand their products again...? From memory it's not because they are quality products, with great results and integrity... Let’s not forget the largest healthcare fraud of all time was committed by Pfizer, who were fined $1.195 Billion.
The Pfizer Vaccine
The only COVID-19 vaccine that has been approved by the FDA is the Comirnaty (new Pfizer) vaccine. However, this vaccine has not been manufactured to the extent where it can be distributed widely and thus it is unavailable at present…
The following can be found on the package insert of this unavailable vaccine:
Myocarditis and Pericarditis “increased risks of myocarditis and pericarditis, particularly within 7 days following the second dose. The observed risk is higher among males under 40 years of age than among females and older males. The observed risk is highest in males 12 through 17 years of age. Although some cases required intensive care support, available data from short-term follow-up suggest that most individuals have had resolution of symptoms with conservative management. Information is not yet available about potential long-term sequelae.”
Limitation of Effectiveness “COMIRNATY may not protect all vaccine recipients”
Adverse Reactions “In clinical studies, the most commonly reported (≥10%) adverse reactions in participants 16 through 55 years of age following any dose were pain at the injection site (88.6%), fatigue (70.1%), headache (64.9%), muscle pain (45.5%), chills (41.5%), joint pain (27.5%), fever (17.8%), and injection site swelling (10.6%).”
The vaccine was approved based on 2 studies completed. After adjusting these results for placebo effects, it turned out that after Dose 1, ~60% of vaccinated persons experienced fatigue, headaches and joint pain predominantly amongst other symptoms such as vomiting, muscular pain and diarrhoea. After Dose 2 was administered, nearly 100% of the vaccinated participants experienced multiple symptoms, especially fatigue.
Other associated adverse reactions detected in vaccinated individuals were:
Nausea
Malaise
Chills
Swelling and Redness
Lymphadenopathy
Asthenia
Decreased appetite
Hyperhidrosis
Lethargy
Night sweats
Bell’s palsy (facial paralysis)
But perhaps the most worrying risk factor for adverse outcomes is Thrombosis and resulting neurological complications and cardiac issues.
So let’s explore this, illuminate why this may be the case and how you can lower your risks.
Thrombosis risk for COVID-19 Vaccination
COVID-19 is tied to an increased incidence of thrombotic and inflammatory events, which contribute to its severe morbidity and mortality. Several anticoagulants appear to have been tried with most MD's using heparin. However, studies have emerged showing that standardized treatment may not be the best path forward if we don't understand the disease caused by the virus SARS-COV-2 well yet.
D-dimer is a protein your body makes in the process of clotting.
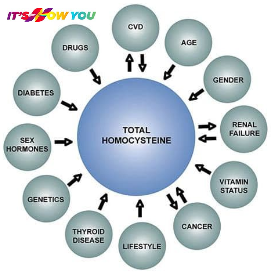
Homocysteine is a sulfur containing amino acid which normally combines with B12, B6 and Folic acid (B9) to work productively in the body. If there are high levels of homocysteine in the blood, this is an inflammatory sign.
Approximately 1 in 3 people have specific genetic modifications, SNP's (single nucleotide polymorphisms), which impede the breakdown of homocysteine, leading to higher blood clot levels and thus increase the risk of thrombosis. However, it is the T allele which is of specific interest in relation to MTHFR C677T, which poses the greatest risk according to the studies.
The following gene activation is associated with homocysteine levels in your blood. If you have single nucleotide polymorphism (SNP) mutations on the CBS, ABO, CPS1, MTHFR, (RPL24P4 and GNMT), and (ALDH1L1 and ALDH1L1-AS2) genes, then the probability of a thrombotic reaction as a result of COVID-19 vaccination may be far greater.
In the study (Geovanni Ponti, et al 2021), “It is known that a high plasma level of homocysteine significantly increases the incidence of vascular damage in both small and large vessels. Hyperhomocysteinemia has neurotoxic, neuroinflammatory, neurodegenerative, proatherogenic, prothrombotic, and pro-oxidative effects. Homocysteine concentrations above the 90th percentile are associated with increased risk of degenerative and atherosclerotic processes in the coronary, cerebral and peripheral circulatory system. In this regard, determining homocysteine together with other cardiovascular risk markers (Apo B, Lp (a), LDL, fibrinogen, PAI-1) now is implemented in the clinical practice and should be tested prior to vaccination; moreover, recent evidence suggests the role of homocysteine is a risk factor for thromboembolism, given its effect on platelet reactivity. This then clearly demonstrates that COVID-19 incidence and mortality rates are strongly correlated to the majority of MTHFR C677 T mutation, which is linked explicitly to prothrombotic events due to altered homocysteine metabolism.”
Do you know if you have the “T” risk allele on your MTHFR C677T gene?
The study went on… There is a clear trend toward the worldwide prevalence of MTHFR 677 T and COVID-19 incidence and mortality. The prevalence of MTHFR 677 T allele in the Latino population, and the incidence and mortality for COVID-19 was higher for this ethnic group than that reported for most other populations globally. Statistical analysis showed a relatively strong correlation between C677 T and death from Coronavirus.

There is a “significant correlation between blood Hcy >16umol/L and severe prognosis or mortality” affected by COVID-19 infection. The study goes on to say, “Some adverse biochemical effects of the thermolabile enzyme coded by the T allele, such as the increase in total plasma homocysteine, appear to be reversible by increasing the consumption of B vitamins and folic acid.” So now we know that not only Vitamin D, Vitamin C, Zinc and Quercetin help protect you from COVID-19 disease, but so do B Vitamins, such as folic acid. A note of caution here, too much folic acid is also not a good thing. Sunlight naturally regulates folic acid levels in the body utilising melanin pigment. In general, if you receive regular sunlight exposure then you should have no issues with too much or too little folic acid. The study concludes by saying: Genetic polymorphism of MTHFR C677 T may modulate the incidence and severity of COVID-19 pandemic infection.
Three other studies also found the MTHFR and homocysteine connection to thrombosis.
Study #1 Conclusion: Our findings indicate that the MTHFR rs1801133 polymorphism may serve as a potential biological marker for venous thromboembolism in Caucasians, East Asians, and West Asians. Moreover, the MTHFR rs1801133 polymorphism may be implicated in the development of deep vein thrombosis and pulmonary embolism, while the MTHFR rs1801131 polymorphism may contribute to the development of pulmonary embolism. https://pubmed.ncbi.nlm.nih.gov/30466296/ NB: C677T is also known as rs1801133. A1298C is also known as rs1801131.
Study #2 Conclusions: The prevalence of variants was greater in thrombosis patients as compared to unmatched controls. Our study highlights the fact that MTHFR C677T polymorphism as compared to A1298C significantly affects Hcy levels in patients with thrombosis indicating that patients with mutant variants are at higher risk of rapid progression of their disease condition. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6759526/
Study #3 Conclusions: Heterozygous or homozygous MTHFR variants, especially a compound mutation, are associated with increased risk of VTE. Hyperhomocysteinemia does not correlate with MTHFR polymorphisms or VTE risk. Hence, MTHFR genotyping provides more consistent assessment of VTE risk. This information can be incorporated into risk stratification for early intervention and prophylaxis of VTE. https://pubmed.ncbi.nlm.nih.gov/29212064/
NB: VTE refers to venous thromboembolism
Bottom Line: It's wise to check for the MTHFR C677T variant along with homocysteine and D-dimer levels in the blood. These will give you a more accurate determination of potential thrombotic events post COVID vaccination. If you have a vaccination appointment set up and don't know your homocysteine or D-dimer levels, you’re risking a possible adverse reaction. If you do know your blood levels of homocysteine, and it’s high, your probability of an adverse reaction may also be higher than others with low homocysteine levels
Homocysteine and Adverse Events
Homocysteine is a key determinant of the methylation cycle’s ability to operate in blood vessels. As homocysteine rises so does IL-6. IL-6 is linked to just about every mitochondrial disease on this planet. IL-6 destroys the redox potential everywhere it is found because it raises cortisol in the stroma of organs. When cortisol is high, collagen is destroyed, it loses its piezoelectric and flexoelectric signalling, while cells get larger in volume and mass. While this goes on simultaneously, homocysteine rises, Vitamin D lowers, and methylation becomes disrupted. Nitric oxide is destroyed and clotting becomes more likely.
· The SAM-to-SAH ratio defines the methylation potential of a cell and is a proxy for the redox potential in the circulatory system. A high SAM-to-SAH ratio is bad.
· Condensation of methionine with ATP, leads to the formation of SAM (S- Adenosylmethionine). The methyl group attached to the tertiary sulfur of SAM can be transferred and therefore can cause methylation of other substances in the body that need it. It is a marker of how energy transfer is accomplished. This methylation is accompanied by energy loss, so this reaction is irreversible. The demethylation reaction leads to the formation of SAH (S- adenosylhomocysteine). SAH is a thioether (a sulfur bonded to two alkyl or aryl groups) analogous to methionine. Methionine is the start amino acid signal in the creation of every human protein. The fidelity of this signal is highly leveraged to redox power in the cell.
· Homocysteine is a key determinant of the methylation cycle and how easy energy is transferred from mitochondria to proteins in the body. Long COVID is likely related to high levels of homocysteine due to poor energy transfers. Homocysteine is methylated to methionine, which undergoes S-adenosylation and forms S-adenosylmethionine (SAM). S- adenosylmethionine is the principal methyl donor for all methylation reactions in cells.
· High Homocysteine —> high Hageman Factor —-> increase platelet stickiness —> Clots.
When homocysteine is elevated, water flows in cells are altered, and swelling ensues, worsening the volumes and mass relationship. Any time these are altered, apoptosis and autophagy programs are altered in the colony of our mitochondria. This is why water has its own specific nuclear footprint when we see cancer on an MRI. There are massive alterations to the Rayleigh Benard cycling of water inside cells. Everyone with sleep apnea (hypoxia) has high levels of IL-6 in the brain which alters the EZ of water in the brain. It correlates 98% of the time with low DHEA levels. This tells us cortisol is being shunted over the sex steroid hormones in response to the homocysteine elevation; i.e. pregnenolone steal syndrome. COVID is a known hypoxia-related disease associated with acute spikes in homocysteine.
DHEA and Sleep are thus linked because of pregnenolone steal syndrome. We can tolerate more inflammation within our brain from a ketogenic diet because our immune system is getting more electrons. Ketogenic diets are all about deuterium depletion of the mitochondrial matrix that improves piezoelectric ability. Ketogenic diets also restore NAD+ by producing more NAD+.
NAD+ has two roles in biology:
It serves as a cofactor in redox and important metabolic reactions in which case it is shuttled back and forth between the NAD+ and NADH forms but is not consumed.
It serves as a signalling molecule in which case it is consumed as a substrate by sirtuins.
NB: NAD+ levels are a proxy for the redox state.
Homocysteine can lead to global DNA hypomethylation and DNA damage. It may also suppress transcription of cyclin A in endothelial cells all associated with oxidative stress. Cell exposure to homocysteine seems to lead to a significant reduction of cell viability, including the length of time homocysteine seems to affect cell viability and how it sensitises them to ROS. Cell exposure to homocysteine for a period of 3 days did not induce any significant change in Reactive Oxygen Species (ROS) levels, but incubation with homocysteine for 5 days resulted in a 4.4-fold increase in ROS production. Several studies demonstrated that homocysteine is capable of triggering neuronal damage via oxidative stress, DNA damage and activation of pro-apoptotic factors in mitochondria in cell cultures or animal models.
The protein p21 (also known as WAF1, CIP1 or SD11) regulates cell proliferation by inhibiting the cell cycle through the cyclin kinase pathway. It also has been shown to inhibit apoptosis induced by numerous stimuli. The longer homocysteine stays elevated the more dramatic p21 up-regulation and protein synthesis seems to occur.
In mRNA vaccine injuries:
SAM-to-SAH Ratio is high
Homocysteine is high
IL-6 is high
Hs-CRP is high
Vitamin D is low
P21 is high
Folate (5 tetrahydrofolate) and Vitamin B12 levels are low
MTHFR C677T is mutated
Key: Improved methionine synthase is the only enzyme in the brain (neural tissue) that is capable of converting homocysteine to methionine.
Data on Vaccine Efficacy
The morbidity and mortality of vaccine adverse events are beginning to add up to be much more significant percentages than we would all like to think about. In Taiwan, as of October 8th, vaccine deaths were higher than deaths from COVID-19. Why are we seeing a global push for mandates on a ‘cure’ that is potentially worse than the disease itself? No wonder Israel and Iceland are furious, as they are vaccinating their entire populations and having worse COVID-19 outbreaks than before the injections were administered.
Do you remember this study from April 2021 on the COVID-19 Vaccine Efficacy and effectiveness Study Results? https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(21)00069-0/fulltext?s=09. Let me remind you of the summary takeaway points:
Absolute Risk Reduction (ARR) of vaccines:
ARR = 1·3% for the AstraZeneca–Oxford
ARR = 1·2% for the Moderna–NIH
ARR = 1·2% for the J&J
ARR = 0·93% for the Gamaleya
ARR = 0·84% for the Pfizer–BioNTech
Not looking good so far…
Let’s take a look at this article from Doctors for COVID Ethics from September 2021. https://doctors4covidethics.org/letter-to-physicians-four-new-scientific-discoveries-crucial-to-the-safety-and-efficacy-of-covid-19-vaccines/. The great thing about this article is it’s 12 citations of studies on COVID from 2020 and 2021. So, they contain the most up-to-date and informative scientific research.
Here’s a summary of what they discovered after analysing the various studies:
Rapid and efficient memory-type immune responses occur reliably in virtually all unvaccinated individuals who are exposed to SARS-CoV-2. The effectiveness of further boosting the immune response through vaccination is therefore highly doubtful. Vaccination may instead aggravate disease through antibody-dependent enhancement (ADE).
Discovery 1: SARS-CoV-2 spike protein circulates shortly after vaccination (Explaining the many adverse events)
Discovery 2: Rapid, memory-type antibody response after vaccination (Severe cases of the disease thus cannot be ascribed to lacking immunity, instead related to ADE because of vaccination)
Discovery 3: SARS-CoV-2 elicits robust adaptive immune responses regardless of disease severity (Therefore, vaccination is unlikely to provide significant benefit with respect to the prevention of severe lung infection.)
Discovery 4: Rapid increase of spike protein antibodies after the second injection of mRNA vaccines (The possible consequences of all-out self-attack by the immune system are frightening)
Conclusion: “The collective findings discussed above clearly show that the benefits of vaccination are highly doubtful. In contrast, the harm the vaccines do is very well substantiated, with more than 15,000 vaccination-associated deaths now documented in the EU drug adverse events database (EudraVigilance), and over 7,000 more deaths within the UK and the US. ALL PHYSICIANS MUST RECONSIDER THE ETHICAL ISSUES SURROUNDING COVID-19 VACCINATION.”
Have you been told that you need a COVID-19 vaccine by your educational institution, school or employer?
In the USA, Australia, UK, Canada and many other countries around the world the ‘emergency use authorization’ is still in place. However, it is only the vaccines which are approved by the FDA, TGA, MHRA, Health Canada and all other medical regulatory bodies which are allowed to be used as medical treatments. That being said, if a medical treatment such as a vaccine is ‘provisionally approved’ it may be used under an ‘Emergency Use Authorisation’ (EUA) despite not being approved. The regulators state that they are rigorously monitoring the safety and effectiveness during the roll-out, however, given the significant adverse events, I find this hard to believe.
In the USA, the FDA has approved the Comirnaty (new Pfizer) vaccine, however it is not available at the moment and the EUA vaccines remain being used. The law is not behind this widespread use and mandate of the EUA vaccines. In fact, it is technically illegal, despite the opinion that the Department of Justice is saying it is allowed.
In Australia, there have only been provisional determinations, no approvals of any COVID-19 vaccines. This means it too is not supported by the law to mandate any of these provisionally determined vaccines in Australia - Pfizer (Comirnaty), AstraZeneca (Vaxzevria), Moderna (Spikevax) and COVID-19 vaccine, Jansse.
Before we go any further with analysing the vaccines, let’s remember that if there is effective treatment of a disease, vaccinations are legally not required. Studies on Ivermectin, Hydroxychloroquine and various vitamin and mineral concoctions are being suppressed, unfunded and buried to keep the vaccine narrative going. Oh wait… here’s one study showing Hydroxychloroquine and Ivermectin’s incredibly effective treatment effects on COVID-19 (https://www.researchsquare.com/article/rs-98106/v1). Dr. Robert Malone “Ivermectin may be able to irradicate COVID-19”. Pat Cash “I’ve been taking Ivermectin for the past year to prevent COVID-19, as have many other professional athletes and coaches.”
Employers have already lost in court against contesting religious exemptions in the USA. South West Airlines and Intel have backed down from mandating vaccinations for employees. But it took employees to stand up and be willing to contest this decision instead of complying in ignorance.
Bottom Line: I would suggest challenging your employer on 1. How are they providing informed consent of vaccination? 2. How are they providing healthcare insurance, life insurance and disability insurance? 3. Where is their legal documentation from the government saying they must mandate these vaccines for employment?
Here’s the employee discloser form which you can give to your employer or school https://home.solari.com/forms/
Ok, so, by now you realise that the available vaccines for COVID-19 have great risks and are being administered without informed consent, safety and efficacy data, and may be illegal if they are said to be mandatory. You also know that there are effective medical treatments for the disease that are being suppressed.
The Pseudoscience of Long COVID
Have you heard of 'Long COVID'? Referring to this article https://www.wsj.com/articles/the-dubious-origins-of-long-covid-11616452583?fbclid=IwAR2QxFzhS_YPeeCHm4tYiyoYlEZFZPo7RxpH0pwZhQmUqh9Uusy2QvZTY-c I have taken some quotes which provide a helpful explanation of the pseudoscience.
"The concept of long Covid has a highly unorthodox origin: online surveys produced by Body Politic, which launched in 2018 and describes itself atop its website’s homepage as “a queer feminist wellness collective merging the personal and the political.”
"Patients who struggle with chronic and vague symptoms often vehemently reject a physician’s diagnosis that suggests an underlying mental-health issue, in part because of the stigma around mental illness and the false belief that psychologically generated symptoms aren’t real.”
"By relinquishing the need for objective serological confirmation, and by claiming that long Covid can manifest in a mind-boggling 205 different symptoms, the Body Politic Covid-19 Support Group offered its readership exactly this attractive alternative"
"The government listened and now will further perpetuate patient denial of mental illness and psychosomatic symptoms. Two days after the NIH’s funding announcement, Solve ME/CFS announced it was launching the Long COVID alliance, which Body Politic shortly joined."
"By drawing attention to and legitimizing the ever-present threat of long Covid, medical authorities will lead a large group of impressionable patients to believe that their Covid-19 symptoms have not resolved and that they are helpless victims of an unrelenting sickness."
"The NIH’s decision is a victory for pseudoscience and will do more to harm than help patients."
So, it appears that if you are healthy: have low inflammatory levels, have a robust immune system, have good gut health, have a strong mitochondrial redox, have good quality sleep, have a well-functioning brain without brain fog, then your risk of COVID-19 being the last disease you will ever have is 0.
Finally, let’s touch on Natural Immunity
True individual and herd immunity only come from natural disease processes... also some people likely have immunity from past exposure to other viruses in the Corona family. It's ridiculous to fear people with natural immunity rather than those whose immune systems have undergone experimental modifications.
Here’s an article explaining that our innate immunity is much more effective than the injection. https://www.news-medical.net/amp/news/20210801/Antibody-responses-following-SARS-CoV-2-infection-more-potent-than-vaccine-elicited-ones.aspx.
Various medical publications have published reports on the findings that natural immunity is stronger than vaccine immunity.
Red flags you should be made aware of:
Waning immunity in Israel & Iceland in the vaccinated.
Unusual high vaccinated hospitalization rates in Israel/Iceland from vaccine variants
Antibody Dependent Enhancement (ADE) developing in vaccinated in Australia and USA
The development of Vaccine-Associated Enhanced Respiratory Disease (VAERD) in the jabbed.
Natural durable cell immunity is best as the PEER reviewed article shows here. https://www.news-medical.net/.../Antibody-responses...
How do you prove Cell-mediated immunity to avoid manufactured immunity therapy mandates?
Lockdowns/Business Loss - Ineffective
PCR Regular Testing for Client - Ineffective
PCR Testing when CLI/ILI Symptomatic - Ineffective
Mask, Distancing, Isolation - Ineffective
Living a Foundational Health Lifestyle such that you get C0V!D and never even know it - Priceless.
You have an immune system, and it works, otherwise you wouldn't be here. Allow your immune system to increase in intelligence by increasing its robustness by spending as much time as you can outside.
Natural Herd Immunity is durable and Never Creates Variants like Manufactured Therapies do.
As Marcus Aurelius would say it, Injustice is committed by doing and saying nothing when you know something harmful is happening.
Stay healthy or you'll become a slave of the 'health industry'.
Medically assisted populations are medically controlled populations.
Stop being so Risk Averse if you are medically healthy.
Ask, why did a seasonal virus Delta spike in summer (the wrong season)...
I'm going back out into nature now... See you there!

Cites:
Research article in Wiley https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8209953/pdf/JCLA-35-e23798.pdf
https://pubmed.ncbi.nlm.nih.gov/32325252/
Dr. Peter McCullough https://www.bitchute.com/video/kZsB8VDWSzCv/?fbclid=IwAR3nQ1X9b3x01tT-bxXrN3aOPlJGS9z0X35K0_F9kY9eFIj0l3VddQlVACQ
TGA Provisional Determination of Injection https://www.tga.gov.au/publication/provisional-determination
Dr Richard Fleming (PhD, MD, JD = Gives a science-based presentation on the pandemic. https://thehighwire.com/videos/live-from-event-2021-in-dallas-tx/
“No relationship between percentage of population fully vaccinated and new COVID-19 case.” https://l.facebook.com/l.php?u=https%3A%2F%2Flink.springer.com%2Fcontent%2Fpdf%2F10.1007%2Fs10654-021-00808-7.pdf%3Ffbclid%3DIwAR2uS6kvkAUGLEkhxYwVt1jDq_xTaOJZczHYRlBa2M5GWjoDQhX_Np5PL3M&h=AT0xvOMFcD7fCaYm5kNamrBd2-n00gpwY63SILNzCrNWIUzK96cGFbpI8egkPBTxWEHh8_3oxtuRQ0_C85iGx6iePbaESRTkJwI5nXaYXfoZxg6S2jtxS-4OSdz6yuGWFn5IpWwNaSIcbqq8SA&__tn__=R]-R&c[0]=AT2dX7nHdTQJZyUyxFIlk4NiiQY1pDHubUbj398paJUQOAHuEZjMXLcdtK4M9KOk11jZkrMW_okpLxcLPdhoD5VNRJGoJPFk0wF_CV9k8rdNLfbFZLKbf59ga2DzEuud45Cs9D0ISQHjbyq9yZicNY9boAw
Sleep, circadian Rhythms and Melatonin Optimisation regarding COVID-19 https://www.frontiersin.org/articles/10.3389/fnins.2021.711605/full?fbclid=IwAR2QxFzhS_YPeeCHm4tYiyoYlEZFZPo7RxpH0pwZhQmUqh9Uusy2QvZTY-c
Taiwan has more Deaths form Vaccination than from COVID-19 itself. https://www.zerohedge.com/news/2021-10-14/deaths-following-vaccination-reported-taiwan-exceed-nations-covid-deaths
Innate immunity protects children against Delta Variant more than the Vaccine https://www.reuters.com/business/healthcare-pharmaceuticals/delta-does-not-appear-make-children-sicker-secondary-immune-response-stronger-2021-10-08/?fbclid=IwAR0Rj-sTdKQsu26rGrWzoUsNFT5zmpk3xQG6gmuZLNvzIKLpKi7VCk2xXIw
Geert used to work for Solvay Pharma in the vaccine division. https://www.youtube.com/watch?v=w3xq4cEHT0s
A PATHOLOGIST SUMMARY OF WHAT THESE JABS DO TO THE BRAIN AND OTHER ORGANS https://www.bitchute.com/video/TsdTTHJteilw/
Dr. Zelenko says Google Executives are taking Ivermectin https://www.bitchute.com/video/c0ROBN0qdLZ1/?fbclid=IwAR2BMogBB_7LiUdh2pGzFyxG0XH9U5Lul8o-1p-PqrksioOlU4ntcN5t-aU
Quantas Piolet Speaks Out About Vaccine Mandates https://www.bitchute.com/video/Ybzcfy0VDk5i/?fbclid=IwAR0nHUThGdg7lzJhjJ5mpJYdYeRtBbNplkrS9tjcwX1irbVa9QawXbM_PUM
Non compliance appears to be the best way out https://www.nomadnero.com/post/kingsland-georgia-9-14-21-noncompliance-is-the-way?fbclid=IwAR1ocNGqbKYCSkgQ_Ok8qOwcN6lWJDmgvnGzpkMEpr_4JRLR6UrJiP-juds
Vaccination Adverse Events Stories https://www.worldtribune.com/unexpected-and-heartbreaking-thousands-flood-abc-affiliates-facebook-page-with-vaccination-horror-stories/?fbclid=IwAR1JAf6YwDF4MOMEJAMmVAKBVlDQQx8SzvSQ5VNlCbeayWR8Bs-ppNhbJ6Q
Dr. Rhonda Patrick on Vaccine Misinformation https://www.youtube.com/watch?v=WB6yucemJ-o&t=276s&ab_channel=PowerfulJRE
The "Virus" Pandemic Is A Farce: Drs. Thomas Cowan And Andrew Kaufman Interviewed by Mike Adams https://www.bitchute.com/video/Zez4gdpUfHEK/?fbclid=IwAR1iVyDCvvYk_EzNspiC_IqhzfGnhQTWx3yMDocWf7WoYwMzyH-IytRK25s
Over 100 Canadian Children Hospitalized after Vaccination https://torontosun.com/news/provincial/over-100-ontario-youth-have-been-sent-to-hospital-for-vaccine-related-heart-problems?fbclid=IwAR0WQvWAO4PNwgx9Rcfk48MWWNFkFpwiuz3Ckf1EkaCDO7Bo5h1uj4beM_E
Antibody responses following SARS-CoV-2 infection more potent than vaccine-elicited ones https://www.news-medical.net/amp/news/20210801/Antibody-responses-following-SARS-CoV-2-infection-more-potent-than-vaccine-elicited-ones.aspx?fbclid=IwAR1Fi0gbOOOqIqiVEXjw_DcdgVGuNCh9oCaeLbhAaK3DSc5zPkOpSWpwbbo
Dr. Robert Malone (inventor of mRNA technology) https://www.youtube.com/watch?v=nYkUePQMfkE&t=1s
Denmark stop all COVID restrictions https://freedomfirstnetwork.com/2021/08/denmark-abolishes-all-corona-measures?fbclid=IwAR3GTstOs8IYzUjNMHAq9Xe26RlNoyWST5daRfbKvYkt2b6eVsrH0GmTxb8
Paul Craig Roberts and Dr. Tess Lawry https://www.paulcraigroberts.org/2021/08/09/the-covid-pandemic-is-a-money-making-hoax-and-perhaps-serves-darker-agendas/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7756688/ and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7467063/
Credit to Bob Moran for the picture at the top of this blog. Check out his art here at his Twitter page https://twitter.com/bobscartoons
Dr. Ted on Natural Immunity https://nationalfile.com/oklahoma-teacher-hospitalised-with-covid-despite-receiving-three-pfizer-vaccine-shots/
Tripple Jabbed man sick with COVID-19 https://noqreport.com/2021/09/30/heres-why-the-vaccines-arent-working/
Hankey GJ, Eikelboom JW. Homocysteine and vascular disease. Lancet. 1999;354:407–13. doi: 10.1016/S0140-6736(98)11058-9. [PubMed] [CrossRef] [Google Scholar]
Loscalzo J, Handy DE. Epigenetic modifications: basic mechanisms and role in cardiovascular disease (2013 Grover Conference Series) Pulm Circ. 2014;4(2):169–74. doi: 10.1086/675979. [PMC free article][PubMed] [CrossRef] [Google Scholar]
Harvey RA, Ferrier DR. In: Lippincott’s Illustrated Reviews, Biochemistry. 5. Rhyner S, editor. Philadelphia: Wolters Kluwer Health; 2011. pp. 264–5. [Google Scholar]
Guo H, Chi J, Xing Y, Wang P. Influence of folic acid on plasma homocysteine levels & arterial endothelial function in patients with unstable angina. Indian J Med Res. 2009;129(3):279–84. [PubMed] [Google Scholar]
Baszczuk A, Kopczynski Z. Hyperhomocysteinemia in patients with cardiovascular disease [Abstract] Postepy Hig Med Dosw. 2014;68:579. doi: 10.5604/17322693.1102340. [PubMed] [CrossRef] [Google Scholar]
Curro M, Gugliandolo A, Gangemi C, Risitano R, Ientile R, Caccamo D. Toxic effects of mildly elevated homocysteine concentrations in neuronal-like cells. Neurochem Res. 2014;39:1485–95. doi: 10.1007/s11064-014-1338-7. [PubMed] [CrossRef] [Google Scholar]
Shenov V, Mehendale V, Prabhu K, Shetty R, Rao P. Correlation of serum homocysteine levels with the severity of coronary artery disease. Ind J Clin Biochem. 2014;29(3):339–44. doi: 10.1007/s12291-013-0373-5. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
Carmel R, Jacobsen DW. In: Homocysteine in health and disease. Carmel R, Jacobsen DW, editors. Cambridge: Cambridge UP; 2001. pp. 183–93. [Google Scholar]
Wuerthele SE, Yasuda RP, Freed WJ, Hoffer BJ. The effect of local application of homocysteine on neuronal activity in the central nervous system of the rat. Life Sci. 1982;31:2683–91. doi: 10.1016/0024-3205(82)90712-3